
Obesity Facts
I’m starting this page to serve as a central repository of significant concrete facts about obesity. I’m making this a page because I anticipate frequently updating it as necessary. There will be no speculative musings or inferences based on partial evidence, everything here will be solid facts as per the research.
Most people who comment on this topic – especially the most vocal – tend to be quite clueless on these matters. This should be a one-stop spot to bring everyone up to speed.
Sections:
Individual-level heritability of obesity
Group-level heritability of obesity
Ineffectiveness of obesity treatments
Laboratory/surgical interventions
Overstated impact of obesity per se on health
Individual heritability of obesity
 Obesity is known to be highly heritable. A meta-analysis of twin and family studies (which included the standard MZ together vs. DZ together – MZT-DZT – in addition to MZ apart, MZA), which looked at a combined total of 140,525 individuals found a heritability of body mass index (BMI) in the range of 0.75 to 0.82. The countries observed included the U.S., Britain, Australia, Denmark, Sweden, Norway, Italy, Finland, South Korea, Taiwan, China, and Japan. The results are highly consistent with little variability across the studies.
Obesity is known to be highly heritable. A meta-analysis of twin and family studies (which included the standard MZ together vs. DZ together – MZT-DZT – in addition to MZ apart, MZA), which looked at a combined total of 140,525 individuals found a heritability of body mass index (BMI) in the range of 0.75 to 0.82. The countries observed included the U.S., Britain, Australia, Denmark, Sweden, Norway, Italy, Finland, South Korea, Taiwan, China, and Japan. The results are highly consistent with little variability across the studies.
If we were to rely solely on estimates drawn from MZT-DZT studies, the matter of whether some sort of environmental factor(s) that serves bias upward heritability estimates would remain. This is addressed by the smaller MZA & DZA studies (included in the analysis). One in particular had a sample of 93 pairs of MZA and 218 pairs of DZA. The correlation was for the MZA (for men) was 0.74 (n pairs = 49) and 0.66 for women (n pairs = 44). All told, the study estimated a broad sense heritability of 0.74 for men and 0.69 for women, with much of the variance being due to non-additive genetic effects.
This is additionally supported by adoption studies. One review of twin and adoption studies (n adopted ~ 1,400) found significant correlations between adopted children and their biological relatives and no correlation between adoptive relatives, at least not in late adolescence and adulthood. In other words, in the adoption data, the heritability was found to be high and the shared environment impact was found to be zero, in agreement with twin studies.
The high heritability of BMI was also confirmed by a genome-wide complex trait analysis (GCTA), which used directly measured genomic similarity to assess heritability. One analysis with 20,240 sibling pairs found that captured SNPs could explain 42% of the variance in obesity. This estimate is a lower bound of the additive heritability only, and then only the heritability explained by common SNPs. This is in agreement with the apparent additive heritability of obesity (0.3-0.4), which appears to be in that range from MZA studies.
Another GCTA, from Iceland, which looked at 38,167 individuals and estimated heritability from both relatives and non-relatives, found a lower-bound broad-sense heritability estimate (additive + non-additive genetic variance) of BMI of 0.471. GCTA results are lower bounds estimates, because they are limited by genetic variants captured by the analysis.
The bottom line is that genes heavily influence individual variation in obesity. It seems some people are incapable of understanding this, but it should go without saying that genetic differences are, however, not involved in the change in obesity rates over time. Genes haven’t changed significantly during the past few decades, so some “environmental” factor(s) must be in play. Please see my post Why HBD for a description of how gross environmental change can lead to gross phenotypic change without any genetic change.
It is also important to note that the shared environment contribution is reliably zero. This means, as is the case with behavioral traits, parents and the family environment have no effect on adult obesity. One cannot blame adult body weight on parental choices etc.
Finally, there is a marked misconception that there is some sort of “debate” about whether body weight is genetic (which it heavily is) or stems from “choices” (i.e., behavior). This is one of those things that’s not even wrong. There can be no dichotomy between “genes” and “choice.” As HBD Chick would put it, where do choices come from? As readers of this blog know, the First Law of behavioral genetics is that all human behavioral traits are heritable. Genes (i.e., specifically, genetic differences) impact all human behavior (i.e., behavioral differences) to some degree. Indeed, often considerably so. More fundamentally, the phony dichotomy between genes and choice stems from a key misunderstanding: the failure to realize that the universe is deterministic. All events, including human behaviors, have causes. (This is even considering quantum mechanics; quantum indeterminacy is merely another “deterministic” force. Random interplay is just another causal agent.) See my post No, You Don’t Have Free Will, and This is Why.
To the extent that behavior (again, specifically, behavioral differences) lead to differences in body weight – whatever extent that is – those behaviors are themselves quite heritable.
Indeed, in the case of “self-control” (which may or may not be causally related to obesity), it too appears to be largely heritable and not affected by the shared environment. One recent study found that 76% of the variance could be attributed to additive genetic factors.
Group-level heritability of obesity
As I’ve discussed previously, there is not much by way of evidence that the underlying nature of differences between groups is all that different from the nature of differences between individuals within a group – with perhaps the effects of highly deprived environments (such as encountered in sub-Saharan Africa and other highly impoverished areas) excepted. Yet there are significant group-wide differences in the obesity rate. As seen in my post A Fat World – With a Fat Secret?, we see a pattern within nations and between them.
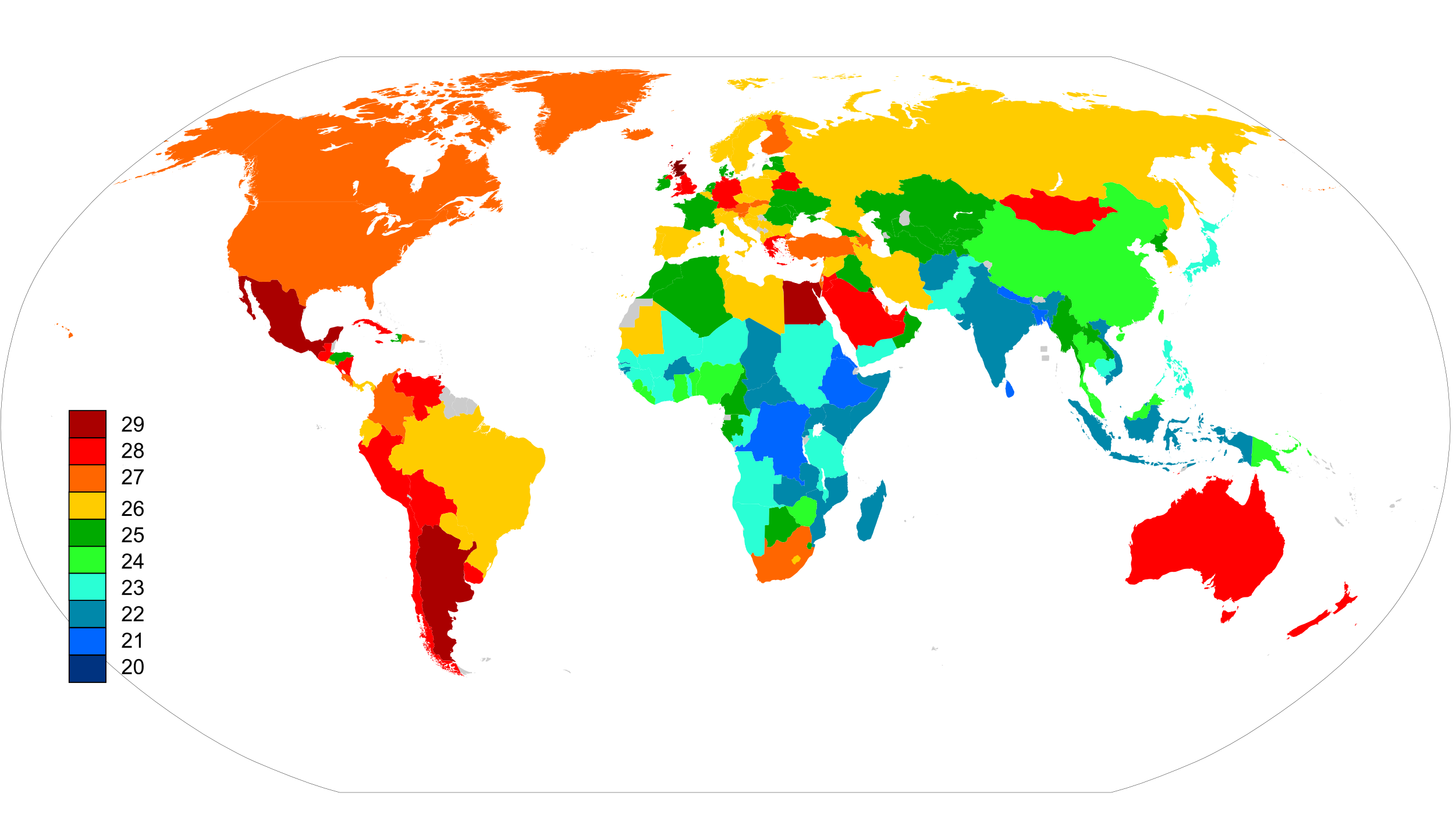 Map of average BMI by nation
Map of average BMI by nation


As discussed in the above post of mine, overall rates of obesity cluster in related groups, even when those groups live together in the same nations. As seen in the U.S., the pattern of ethnic clustering is visible among American Whites, as seen by this estimate of county-level White obesity rates by Razib Khan (blue = higher; red = lower):
 The obesity rate heavily tracks area of Scot and Scots-Irish ancestry – and secondarily, German ancestry, in line with the high obesity rates in Scotland and Germany, respectively. See my posts HBD is Life and Death and More Maps of the American Nations.
The obesity rate heavily tracks area of Scot and Scots-Irish ancestry – and secondarily, German ancestry, in line with the high obesity rates in Scotland and Germany, respectively. See my posts HBD is Life and Death and More Maps of the American Nations.
The evidence strongly indicates that group-level differences in obesity are highly heritable, just as is individual variation in obesity – founder effects and selective migration (and, in the developing world, extreme deprivation and dietary incompatibility) notwithstanding.
Ineffectiveness of obesity treatments
Obesity is very difficult to impossible to treat. The most common prescription, and indeed the prevailing conventional wisdom, is that “lifestyle” changes are the best solution. This typically means diet and exercise. However, this has been extensively studied. Across the population, diet and exercise, each individually and in tandem, are completely useless to treat obesity, in the long term.
In the case of exercise, randomized controlled trials (RCTs) don’t even show a short-term benefit. One 2007 meta analysis by Franz et al looked at the results of all sorts of different interventions. For exercise-alone prescriptions, it found that the treatment groups lost no weight at 6 months (well, less than 2 kgs, but even this number comes only when you look at those who remained in the study). Indeed, after a year, the control groups actually lost more weight than the treatment groups. The total weight change was small and close to zero throughout.
In the case of diets, particularly the most common low-fat and low-calorie diets, a very large meta-analysis of RCTs with a combined N > 60,000 (of which ~48,000 came from a single mammoth trial) and a study duration of 2.5 – 10 years, found that diet was completely ineffective for weight loss. The subjects showed no aggregate permanent weight loss at the end of the study period. The largest of these studies, the one by Howard et al (2006) found little change, a total loss (over 3 years) of less than 1 kg (and a difference between control and treatment groups of 1.29 kg, favoring treatment).
As for diet and exercise combined, several studies in both previous meta-analyses look at trials which tested both together. The result was the same: little to no significant aggregate weight loss, especially after longer periods of time.
This is true of low-carbohydrate diets as well. One meta-analysis looked at RCTs. Each of the trials were individually small (n = 11 – 153), but all told there were 712 subjects in the low-carb trials. The duration of studies ranged from 12 to 24 months. The total average weight lost with the low-carb diet groups was on the order of 4 kg! And that’s with considerable attrition in the studies. Low-carb diets don’t work much better, either.
A new randomized comparison trial (Bazzano et al, 2014) of a low-carb vs a low-fat diet (N = 148) found only a weight loss of 5.3 kg after 1 year with the low-carb diet, but only 1.2% change in body fat percentage.
The results are visualized in this graphic from Franz et al:

Drugs designed to treat obesity often don’t fare much better in trials, as seen with the drugs examined here.
Randomized controlled trials are necessary to judge the efficacy of obesity treatments, especially when crafting broad prescriptions for treatment. Popular conceptions of weight-loss – even in the minds of medical professionals – are biased by odd examples of individuals with impressive short-term weight loss or rare individuals who managed to maintain a lowered weight for a long period of time. This is obviously improper, because it ignores the fact that these individuals are exceptional. The efficacy of any treatment, especially one that is to be recommended as a general prescription to treat any condition, needs to be subjected to clinical trials to judge their effect across the population to which the treatment is intended. This is what we do for new drugs.
However, even these have their limits. RCTs of lifestyle modifications are plagued by considerable non-compliance, even for those who remain in the study. This is especially acute towards the later parts of the longer trials. Some commenters correctly point out that this weakens any conclusions we can draw because we don’t know what the results would be if the subjects stuck to the trial.
However, I argue that this point, as technically true as it might be, is ultimately wholly academic. Patient non-compliance is an important part of the study, because these people aren’t going to live their entire lives in a laboratory under tightly controlled conditions; they are going to live their lives in the real-world feeding and exercising at their own accord. If dietary changes and exercise fail thanks to non-compliance – a point which is not at all clear at the moment, mind you – then they are useless as prescriptions to treat obesity en masse. It does no good to give advice that most people can’t stick to, assuming that non-compliance was the point of failure.
Laboratory/surgical interventions
There has been quite a bit of in-lab based obesity experimentation. Among the most interesting studies out of these are overfeeding experiments. These are experiments where subject are deliberately overfed for some period of time. The best of these confine subjects to a laboratory for the duration of the experiment. The subjects are monitored extensively during that time. Because of the expensive nature of these in-patient trials, they always have tiny samples. A review such studies can be found here:
Joosen & Westerterp (2006) Energy expenditure during overfeeding
One of the best studies used pairs of identical twins (Bouchard et al, 1990). Twelve pairs of identical twins were kept in a lab and overfed for three months. All the twins gained some weight. However, there was a marked variation in how much weight each subject gained. But, more strikingly, there was a tight correlation between co-twins in weight gain:


Both the total weight gained and the distribution of that weight was strongly correlated between twins. Despite the small sample, this is a poignant demonstration of both the great degree of individual variation in propensity to gain weight – even in the same broad conditions – and the genetic underpinnings of such variation.
Even more interesting is the follow-up of these twins (Bouchard et al, 1996). As is the case with most overfeeding experiments the subjects returned to their pre-study weight following their release (however, there was some attrition in the follow-up, so it’s unclear how much that affects these results):

That change was also genetically directed:

 There was some long-term weight gain here, but because there were no untreated controls, it is unknown how much that differs from the general population.
There was some long-term weight gain here, but because there were no untreated controls, it is unknown how much that differs from the general population.
Overstated impact of obesity per se on health
Epidemiology has shown that obesity is associated with a myriad of adverse health outcomes. Epidemiologists have thus proclaimed that obesity is directly causal to those negative health outcomes. This conclusion is faulty for a key reason. As described by Gary Taubes (emphasis mine):
Another problem endemic to obesity and nutrition research since the second world war has been the assumption that poorly controlled experiments and observational studies are sufficient basis on which to form beliefs and promulgate public health guidelines. This is rationalised by the fact that it’s exceedingly difficult (and inordinately expensive) to do better science when dealing with humans and long term chronic diseases. This may be true, but it doesn’t negate the fact the evidence generated from this research is inherently incapable of establishing reliable knowledge.
The shortcomings of observational studies are obvious and should not be controversial. These studies, regardless of their size or number, only indicate associations—providing hypothesis generating data—not causal relations. These hypotheses then have to be rigorously tested. This is the core of the scientific process. Without rigorous experimental tests, we know nothing meaningful about the cause of the disease states we’re studying or about the therapies that might work to ameliorate them. All
we have are speculations.
I have discussed the matter previously in my posts, particularly my posts Obesity and IQ and IQ and Death. As recounted there:
The suspicion dawned on me that the connection between mortality and obesity could be mostly, if not entirely, a result of IQ.
And sure enough, I found something that strongly suggested this. It turns out that the venerable Satoshi Kanazawa did a study that found, in a White British sample, IQ measured in childhood predicts obesity at age 51. I discussed this in a post, that is currently experiencing decent readership thanks to the Geoffrey Miller fiasco: Obesity and IQ
The next logical step was to ask the question of how well IQ correlates to shortened lifespan. And I did that with my 99th post, IQ and Death. Looking at a meta-analysis of several studies of IQ and mortality, it was found that IQ is associated with longer lifespan. Indeed, at least one study in the meta-analysis did look at other possible attenuating factors. It found that IQ was by far the strongest predictor of death. Indeed, “marital status, alcohol consumption, systolic and diastolic blood pressure, pulse rate, blood glucose, body mass index, psychiatric and somatic illness at medical examination) was negligible (10% attenuation in risk)!”
The association between obesity and shortened life, and perhaps most health problems, is mostly, and perhaps entirely, a result of obesity’s association with IQ. As I have noted, and as I have been embroiled in a little controversy over, the “conventional wisdom” on diet, exercise, obesity, health, and death is pretty much bullshit.
Bolstering this point, and much more important from a practical standpoint, is the failure of interventions targeted obesity to produce concrete improvements in health or extension of life. As reported in Tomiyama, Ahlstrom, and Mann:
The diets did not appear to meaningfully lower lipid levels, and accordingly, improvements in coronary morbidity/mortality and stroke were minimal. In all five studies that reported on these outcomes (Hanefeld et al., 1991; Howard et al., 2006; Miettinen et al., 1985; Sone et al., 2010; Whelton et al., 1998), the diets did not lead to significant reductions in coronary morbidity or mortality. Furthermore, in only two (Miettinen et al., 1985; Sone et al., 2010) of the five studies did the diet lead to significant reductions in stroke, and the researchers for one of these studies (Sone et al., 2010) noted that the significant finding should be treated with caution, as there were no group differences on most of the risk factors
for stroke.Overall, there were only slight improvements in most health outcomes studied. Changes in diastolic and systolic blood pressure, fasting blood glucose, cholesterol, and triglyceride levels were small, and none of these correlated with weight change. There were also very small effects of these diets on lipid-lowering medication use and coronary morbidity and mortality.
The much hyped PREDIMED trial from Spain (Estruch et al, 2013) of the “Mediterranean diet,” which claimed to find a reduction in cardiac deaths in the treatment group, failed to make a significant reduction in all-cause mortality. This is addition to the many other methodological problems with this trial (like stopping early).
Additionally, there is the Look AHEAD RCT (also here) of diet and exercise on diabetics in the U.S. Its findings are summed up here:
The study randomly assigned 5,145 overweight or obese people with Type 2 diabetes to either a rigorous diet and exercise regimen or to sessions in which they got general health information. The diet involved 1,200 to 1,500 calories a day for those weighing less than 250 pounds and 1,500 to 1,800 calories a day for those weighing more. The exercise program was at least 175 minutes a week of moderate exercise.
But 11 years after the study began, researchers concluded it was futile to continue — the two groups had nearly identical rates of heart attacks, strokes and cardiovascular deaths.
[…]
But the outcome is clear, said Dr. David Nathan, a principal investigator and director of the Diabetes Center at Massachusetts General Hospital. “We have to have an adult conversation about this,” he said. “This was a negative result.”
The nature and implications of these findings, which is rather damning considering the conventional prescription for heath, is captured well by Tomiyama, Ahlstrom, and Mann:
We believe the ultimate goal of diets is to improve people’s long-term health, rather than to reduce their weight. Our review of randomized controlled trials of the effects of dieting on health finds very little evidence of success in achieving this goal. If diets do not lead to long-term weight loss or long-term health benefits, it is difficult to justify encouraging individuals to endure them.
Pretty much says it all.
Well, there you have it. The matter of obesity is one that is deeply personal and brings out powerful emotions in people. This is to the point that it clouds people’s reasoning and ability to look at the matter rationally. The overwhelming weight of the evidence speaks to considerable genetic involvement in obesity, both on the individual and group level; to the lack of a causal effect on health or lifespan; and to the total failure of interventions – especially the two most commonly prescribed ones – diet and exercise – to significantly impact it. As well, even as such, the evidence makes clear there is little impact on health from these inventions, which – considering the material and emotional cost – makes them less than useless.
Indeed, this video (thanks to a slick commenter) from College Humor perfectly captures the situation:
In this edition of this page, I have forgone talking about surgical interventions. For now, I will say the evidence isn’t looking too good there, either. Future updates will review the evidence on bariatric surgery, as well as new findings as they come to my attention.
Note: Critical commenters that make it obvious that they did not read the page face the prospect of being permanently banned on the spot. Please read the relevant section of this page carefully before raising your objection
97 Comments
Leave a CommentTrackbacks
- The Fat Facts – A New Page | JayMan's Blog
- linkfest – 09/28/14 | hbd chick
- M’n huidige interesse: Human Biodiversity | Alfa NL
- Theory: Americans are fat because we don’t eat enough | evolutionistx
- 200 Blog Posts – Everything You Need to Know (To Start) | JayMan's Blog
- “Ethnic Genetic Interests” Do Not Exist (Neither Does Group Selection) | JayMan's Blog








Hello Im back,
What is the heritability of muscle mass and body fat? Every male I know that has worked for more than ~6 months has had significant changes in muscle mass and body fat…
@Live-Evil:
Good question. I’ll look it up.
There’s at least two points of self-selection there…
It would be interesting to see your coverage of the IQ-physical activity correlation. The evidence seems robust to me, but perhaps you would differ.
@Albert Richman:
Feel free to hook me up with some studies.
Eventually I will add to this page data on the key metabolic differences between the obese and the non-obese.
This all just shows why we need a space program. It is the only environment where we could test the impact of diet on weight without people being able to mess it up by keeping a chocolate bar in their desk draw.
Given that tendency, none of this casts doubt on the power of dietary changes to alter weight. Instead it just shows that we are unable to make voluntary, long term changes for ourselves. That still leaves various tactics which might alter the environment faced or restrict our choice set over the long term based on a single short term decision. It also leaves government action to change the environment and incentives we face.
As a lover of personal freedom and autonomy I’m not especially pleased with this conclusion, but the results are already in… long term I won’t be able to use any of this knowledge to alter my actions anyway.
@strongsloth:
Since the only real impact from obesity is aesthetic, why would curbing it be such a priority of governments that they would need to go to such great lengths?
As Jayman points out above, trying to control the public’s weight would really be largely an attempt to improve general aesthetics masquerading as concern for public health. Also, the government has failed to control what people choose to drink, choose to take for recreational pleasure, and whether to purchase or sell sex. The gov did manage to create large black markets and cause a good deal of suffering from the violence and incarneration steming from the failed vice criminalizations in all of these cases.
@Jay, Ed
My comment wasn’t meant to mean that I think the government should try to control what we eat. I just meant that it is a strategy that doesn’t suffer from the weak (individual) willpower problem.
I’m open to the idea, but not necessarily satisfied of it, that obesity has no negative impact on long term health and life span. That might just be because I haven’t seen the evidence.
What is for sure though is that obesity has negative impacts on health and quality of life short term. Being slim (and being fit for that matter) just feels better and allows people to do things that obese people can’t do. Surely that is worth something.
@strongsloth:
Well, it’s all there above for you. Take a look.
Cost and benefits. Trying to curb obesity will incur significant costs. That’s even assuming that there is any government policy that would work. Proof-of-concept is lacking. Would any putative benefits be worth these costs?
JayMan, you’re conflating the question of whether diets work with the question of whether dietary interventions work. No, nagging overweight people to diet and exercise doesn’t improve their health. And this is an important fact to bring to public attention, because it proves the futility of the tough love and personal responsibility approach to obesity.
But you can’t conclude that weight loss doesn’t improve health, just because non-surgical weight-loss RCTs don’t show improvement. Because as you point out, those RCTs don’t produce much weight loss to begin with. Surgical interventions, that do cause major weight loss, *do* mitigate obesity related conditions [1]. Bariatric surgery may not be worth the complications, but it serves as a pretty convincing demonstration that the problems associated with obesity are actually caused by obesity. Not that the correlations, combined with the often extremely obvious mechanisms (e.g. for exacerbating joint degradation), shouldn’t be convincing on their own.
And you also can’t conclude that there’s nothing we can do, either as individuals or society, to control our weights, just because RCTs in free living populations can’t produce a large difference between control and intervention groups. You can only conclude that whatever it takes can’t be easily randomized. People who lose a lot of weight and keep it off do exist [2], and they do it basically the way that the despised “conventional wisdom” would have you expect. Yes, they’re rare, but that’s actually to be expected if the conventional, behavioral account of obesity is completely true. What are the odds that someone who engages in behaviors that cause them to become obese over the course of years, is going to permanently reverse those behaviors? *Especially* if it was common knowledge all along what those behaviors were?
All this fits in with your thesis that there is no free will: no ghost in the machine that will allow us to break with all previous cause and effect and suddenly start eating right and exercising, because of “willpower”. Anyone with the inclination to do so already does. But that doesn’t rule out the possibility that policy interventions aimed at changing behavior could work. For example, excise taxes and subsidies on foods could totally work, since that intervention is based on sound economics rather than some hand-wavy “personal responsibility” mechanism.
Correlations with IQ and genetics are irrelevant here, because it’s likely that the mechanisms by which genetics influence weight are mediated by behavior.
[1] https://my.clevelandclinic.org/Documents/Bariatric_Surgery/schauerbest.pdf
[2] http://www.nwcr.ws/Research/default.htm
@Nathan:
Quite right.
The key problem is, as I’ll discuss when I add the section of bariatric surgery to the page, is that we don’t actually know that, because there are no RCTs on bariatric surgery! Patients chosen for surgery aren’t a random cross-section of obese people.
Even if that’s quite, which I grant is quite plausible, and even the fact that the causal efficacy of bariatric surgery is not established notwithstanding, it doesn’t follow that obesity is causal to whatever other comorbidities that exist.
Sure they exist. But they’re rare. And what good is knowledge of that fact to everyone else?
Assuming behavior is the problem.
As I said, we can’t make that claim. On what basis are we to establish that this is the likely explanation – not merely possible, but likely?
when i eat a lot i got fatter and when i stop to eat a lot i get thinner, i once lost 7kg in a month because i barley ate anything so from my point of view it sounds really logical that if a person X will cut his daily calories consumption by 20% he will probably wont stay the same weight after two months for example. another example is big looser where really obese people lost a LOT of weight in a short time.
in my opinion most of the participants in the studies you posted just gave up mentally on their diet at some point(because they are lazy) and that’s why they regained the weight they have lost.
@Andrei:
Right, all >60,000 of them, or at least enough of them that the net weight lost was ~0. I guess that makes you one really special snowflake.
Except that’s not actually the case. I’ll add this to the page soon, but direct laboratory experiments with both thin and obese people has shown that the body resists change in weight even with food consumed is tightly controlled.
Note to future commenters: no more comments on the above point until I add that section to the page, please. Thanks.
The compliance issue is interesting. This is one of the reasons rats are often used as proxies for humans in experiments – because you have 100% control over the rat. It won’t do or eat anything that you don’t want it to. With actual humans (especially in a long-term experiment) often all you can ethically do is give them instructions and pray that they don’t knock your experiment into a cocked hat.
but direct laboratory experiments with both thin and obese people has shown that the body resists change in weight even with food consumed is tightly controlled.
America’s Biggest Loser had one contestant gain 2lbs when on a salad only diet which shocked the “experts” who had never heard of the “Milgram?”* study.
*Experiment in prison whereby prisoners were told they would have their sentences cut if they could get to be 20% overweight. Most people could not do it as the more calories they got the more calories they burned up.
The Big Show is the only WWE wrestler who is heavier than Cristina Briggs!
@JayMan
See bodyweight set point.
http://www.obesityaction.org/educational-resources/resource-articles-2/weight-loss-surgery/body-weight-set-point-what-we-know-and-what-we-dont-know
Why is Illinois such an anomaly? Did they not have enough data?
@Patrick C. Wentz:
Good question. The map is not totally reliable because it’s not a direct county-by-county measurement, but an estimate based on state-level data. See Razib’s reasoning in the post.
Interesting post.
This is a subject where you’ve really got to read the studies – there’s always important details that don’t make it into the abstract. For example, people used to believe in a post-workout “anabolic window”, where your body is unusually primed to synthesize protein into muscle after weight training.
So far, so good. But the studies backing this up had an important caveat…they were almost all done on fasted individuals (ie, people who hadn’t eaten in the past 24 hours, or whatever.) This is NOT a usual situation for an athlete. But gym bros who eat six times a day are still convinced that the anabolic window is all important.
http://www.jissn.com/content/10/1/5
“Since the only real impact from obesity is aesthetic, why would curbing it be such a priority of governments that they would need to go to such great lengths?”
There is the issue of subjective well-being. Personally I feel great at a low weight, and I think especially women feel horrible at a high weight.
I guess that depends on the competition. I don’t think women in slim countries report higher SWB than in obese countries, but I don’t know what to adjust for to find something close to a ceteribus paribus.
first commenter here…this was surely an enlightening post but i’m still not conviced that obesity is not an environmetal cause. especially, i’m missing data on obesity in time and income groups. i remember from college, we discussed food processing cost in time and it correlated well with obesity rates rise, at least in the US. with regards to that, i also recently read an article by gregory clark about social mobilty in the US(american dream is an illusion…i think), it’s point basicaly was that the rate was very low among low income immigrants.
so my question is, couldn’t the heritability correlations be just skewed in that low income, junk food environment?what if you would place a low income kid with fat parants up to addoption into a better environment?
i would also be interested in the cost of the diatery treatments and social status of the treated(although not eating sounds pretty cheap to me),but i am aware that such data cannot be easily recovered.
On the health impact, i remember you once wrote, with regards to the gay germ hypothesis, that gay shaming could be a natural defensive trigger. couldn’t fat shaming be analogous?
IQ links well to income and BMI intragoup sure, but that doesn’t mean there can’t be a BMI policy for the less IQish.
@sainchuck:
As I said before, the high heritability of obesity is also found in adoption studies and studies of twins raised apart.
They were very few obese people in the recent past. Also, what would shamers have to gain, in terms of fitness?
You have to find one that works, first.
thank you for the quick response.
ok on second thought the heritability makes sense. offspring of obese mothers have an increased risk for obesity and diabetes and other developmental problems. there are lots of studies on this topic. but doesn’t that than answer your question about what would shamers have to gain, in terms of fitness?(beside more healthy offsprings)
a better question: if we accept the premise that healthrisks are overstated and treatment is futile, do you see any drawbacks beside a shorter lifespam(which doesn’t necessarily mean less offsprings) to being obese? did pixar get it right in their vision of mankind in Wall:E?
@sainchuck:
You’re still not quite getting it: obesity probably doesn’t lead to shorter lifespan, either. Remember, all of that wisdom is based on nonsensical correlational studies.
I see no inherent downsides to obesity, other than appearance, so far. We the people who are now obese more energetic in the past when they were thinner? Has anyone tried to answer that question?
“I see no inherent downsides to obesity, other than appearance, so far. We the people who are now obese more energetic in the past when they were thinner? Has anyone tried to answer that question?”
I don’t see why they wouldn’t be. It’s just physics. Moving a 200lb mass around is easier than moving a 300lb mass around.
@MawBTS:
I think our experiences with the development of obesity and such should caution us from naively applying simple “physics” to the matter.
“I guess that depends on the competition. I don’t think women in slim countries report higher SWB than in obese countries, but I don’t know what to adjust for to find something close to a ceteribus paribus.”
This is probably more at the individual level. They can’t get much satisfaction from being skinnier than women in some other country, but from being skinnier than friends, colleagues etc. Obesity is also linked to other factors likely to influence happiness, like for instance socio-economic status, but it shouldn’t be so hard to adjust for things like that.
As one of the exceptions (lost 50+ pounds 40 years ago and kept it off), I’m sure that obesity is mostly genetic, but that it can be overcome. I lost the weight, and kept it off, the traditional way, by PERMANENTLY eating less every day -ie. changed my lifestyle just like you were told to do (if you use the phrase “going on a diet” you have already lost).
The remarkable thing to me is the small amount of food I need daily to maintain my correct weight. Most people cannot eat this little every day (either because they want to eat more, or because of societal pressure). I cite societal pressure because, as a guy, I’ve repeatedly been kidded about the small amount that I eat. On social occasions, or Club meetings, where people eat together, my friends make fun of the (small) amount that I eat, which is admittedly small compared to others. I laugh it off because (1) I am a man and can laugh at myself and (2) I prefer being slim to eating more. At 61 I can take off all my clothes, stand in front of a mirror, and feel ok about how I look.
I think nurture plays a role this way: (1) The ordinary servings we see in America (and some other places) are too large for people with genetic metabolisms similar to mine and (2) there is an expectation, at least for men, that they eat LIKE MEN, ie. too much for people like me.
I did also exercise more, but don’t think that contributed to weight loss (but did make me more fit). I don’t think many people can eat like I do – small to medium sized meals, no snacking, moderate drinking.
Above all anecdotal but submitted for what it’s worth.
@Tank:
Here’s the key problem with that logic and I have to nip it in the bud here: change is heritable too:
Must be careful with that word nurture. It doesn’t seem like you mean parents and the childhood family environment (the effect of which on obesity is 0).
Congrats that you have achieved a state you’re satisfied with. The problem with generalizing from exception is that they are exceptions, so generalizing from them is difficult.
Jayman
To be clear. I’m not saying that I changed my metabolism, but that I accepted it and found a way to manage it. I think others could do this, but won’t, in part because of (see below and above). Probably also because, genetically, they are not able to do that.
You’re right that nurture was the wrong word. Maybe environment (I mean in the societal sense) (large normal portions; jokes about a “small” appetites).
What’s your idea on antipsychotic-induced weight gain? Obviously psychiatric diseases are heritable, but medications that treat those illnesses are an artificial, man-made device. I take them and I am fatter than anyone in my family. I am seeking to take a certain medication that reduces weight and I am also trying to exercise regularly. Is that just a hopeless endeavor?
@Chuck:
Sure, it seems quite plausible a priori that drugs can lead to weight gain. Looking at the clinical trials would quantify how much.
Exercise by itself doesn’t seem to do anything at all in aggregate (not even temporarily).
If we agree that genotypes allow for a set phenotypes, themselves each dependent on specific environmental interaction, then how does “shared environment” tell us anything? To see what effect the environment actually exerts, we would need to see identical genotypes in non-shared environments. And before we bring up “twin reared apart” studies, let’s note that those families — by and large — probably provide markedly similar environments; after all, the parents who are able to adopt are screened for similar criteria.
Hur, Y., McGue, M. & Iacono, W.G. (1996). “Genetic and shared environmental influences on leisure-time interests in male adolescents.” Individual Differences 21(5): 791-801.
Both genetics and shared environment (e.g., growing up in the same home) contribute to individual differences among adolescent twins’ interests and leisure-time activities, but more than half of those differences are influenced by the twins’ non-shared environment (e.g., having different friends or experiences). Shared environment seems to have a greater influence on activities such as TV viewing, dating, and social activities, than on skill-based activities, like sports, outdoor activities and crafts.
I’m open to being “educated,” but from everything I have read here, the case seems a bit overstated — or maybe that’s just me reading too much fatalism into what you have written. For example, if X result can be achieved with a wide range of genotypes, dependent on certain environmental factors, then parents can greatly aid their children by finding those environmental conditions and immersing the child in those environmental conditions: a guided environmental-match-to-genetic-mix.
The same applies to obesity. There is a reason fitness gurus discuss the endeavor as a “lifestyle change.” They are saying that you must change your entire environment if you hope to succeed. Most individuals fail to keep off the weight because they fail to significantly change their lifestyles.
Maybe you could say “the ability to change” or “motivation to change” is heritable. Perhaps, but “shaming” seems like a reasonable way to alter this phenotype as well. Anyway, I’m open to an education.
@Insider:
I recommend reading these posts: The Son Becomes The Father
More Behavioral Genetic Facts
Or different genotypes in highly similar environments, i.e., adoption studies. Or genotypes of varying relatedness in similar environments (sib-adoption/virtual twin studies, standard twin studies). Look, it’s rather ridiculous to think that in order to gauge the effect of the “shared environment,” the environments children growing up together share need to be identical. They don’t. They just need to be more similar than that of children who didn’t grow up together are. And they are. For the same reason, reared-apart twin studies work.
That depends greatly on what “X result” is, doesn’t it, and how loosely you define it, yes?
Except that exhaustive study has failed to find such an effect.
OK, so do you think you’re a special snowflake?
That’s predicated on the idea that sufficient behavioral change will do the trick. That’s no at all clear at this point.
There’s no evidence for that, either.
‘Or different genotypes in highly similar environments, i.e., adoption studies.’
Yes, but if there is a significant non-shared environment component at play here, and the effect of shared environment decreases with age but non-shared environments increase with age….it seems that, at the very least, non-shared environment may account for some of these differences in “result.”
If you set up the experiment to only view shared environment (or really childhood shared environment + measurement error) and “genetics,” then aren’t you discounting non-shared environment?
Are there studies that look into things like “similar adult peer groups” and “similar non-family experiences” with people of different genotypes? I understand that your view would be that “birds of a feather flock together.” Has this been established?
‘Look, it’s rather ridiculous to think that in order to gauge the effect of the “shared environment,” the environments children growing up together share need to be identical.’
Maybe I somehow misspoke. I actually was referring to the effect of non-shared environments.
‘That’s predicated on the idea that sufficient behavioral change will do the trick’
You mean the behavior of simply eating less calories per day? That is what I take this statement to mean. Can you expound?
‘There’s no evidence for that, either.’
Well, then correct me if I’m wrong, but a proclivity for smoking cigarettes seems heritable. The number of smokers has dropped over the last 50 years. A huge shaming campaign re: smoking took place over that amount of time. Further, several laws were passed that made it more and more difficult for individuals to purchase cigarettes and smoke cigarettes in public.
I only ask these questions because I haven’t found direct answers to them in the materials you have provided.
@Insider:
All current evidence is pointing to the “non-shared” environment being mostly (what isn’t actually measurement error, that is) developmental noise.
Look, think about it: if nothing in the great expanse of environmental factors children growing up together share makes them more similar, why on Earth would we expect such factors to make them more different?
Yes. Are you going to actually read the links I point you to before commenting? I would suggest that you do.
Please reread the page here. If all known interventions, save surgery (which itself is questionable thanks to the fact there is a paucity of randomized trials) fail to lead to weight loss, including reducing caloric intake, why are you so sure behaviors are the key.
The rate of smoking has since remained stubbornly constant since the initial decline.
In any case, this is apples and oranges. See above point.
Oh, my mistake. I now see this entire topic on the More Behavioral Genetic facts page. All right, I will give it a read before I come asking more questions on non-shared environment.
‘including reducing caloric intake, why are you so sure behaviors are the key’
A notorious amount of diet studies rely on self-report data, though. The review you posted didn’t say what portion of the studies it analyzed were based on self-report data regarding compliance. Self-reporting data, in the context of dieting, may be extremely unreliable: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0076632
So, it still may be a question of motivation rather than the actual ineffectiveness of the intervention.
‘The rate of smoking has since remained stubbornly constant since the initial decline.’
https://encrypted-tbn1.gstatic.com/images?q=tbn:ANd9GcRbTuzTZOyhjEG9TQ9aiwKDe5jX1uNabWl4JGJ427owjqih0idm
To me the graphs show a slowing but continued downward trend.
It could be apples in oranges in that one doesn’t respond to intervention, or it could be apples in oranges in that defects in methodology that plague the measurement of intervention in one failed to do so in the other. Do you think that’s reasonable?
@Insider:
My conclusions are based on randomized controlled trials. As explained on the page, noncompliance may be affecting the result, but we must keep in mind any intervention needs to not just work in a lab, but out in the real world. If people en masse are unable to stick to a diet, it is useless regardless if it works in theory.
As I noted earlier, given that the only potential gains from trying to enact strict measure to curb obesity would be aesthetic – assuming that it’s even possible at all – and would come at considerable cost, it is not worth attempting.
Randomized controlled trials can still and often do use the “free living” methodology, which is a methodology that relies on self-reporting.
And your comment regarding what needs to work in the real world gets back to my original comment about motivation. You were questioning whether any behavioral changes could be effective. In studies where participants are more closely monitored (non-free living), calorie restriction leads to weight loss. So, this seems like an effective behavioral change.
The question still seems to come back to how people can be motivated. Research that has focused on shaming has treated shaming as a one rather than two part affair. Shaming includes bias against the targeted condition and positive reinforcement for all actions taken in opposite of furthering that condition.
—-
Also , as I go through the literature your posts directed me to, I haven’t been able to find your position on the fact that g itself is set up definitionally as a common factor between multiple metrics. So it seems tautological to argue that g is the common factor explaining x or y because definitionally it is a measure of the positive correlations between x and y. Superficially, g seems like a weak indicator of causal relationships. And it seems like the individual metrics have significant partial correlations with one another.
Just direct me to what your position on this is so I can read the literature fully informed. Thanks.
@Insider:
The key point here is that any intervention that is expected to be effective in the general population will require voluntary adherence by the subjects. Hence, to ask if diets can lead to weight loss under laboratory conditions is the essence of an academic question. The answer is yes, but can this be then translated into something that people will voluntarily adhere to? The answer to that so far seems to be no.
Again, even if this would work – which is not at all clear – why is it worth trying?
In the future, please direct all off-topic questions or comments to a relevant post/page or to my Open Thread. I will answer your remaining question there.
Well first I needed to address a statement of yours:
So-called “lab” studies have shown us that certain interventions do work. “Free living” studies only show us that telling people to follow diet X and leaving them to their own devices is ineffective for weight loss.
I fail to see how it’s merely an “academic” question: the only way to know what interventions, if followed, actually work, is to test those interventions under laboratory conditions. There are two steps here — first, figure out what diets or behaviors actually result in weight loss; second, figure out what “diet advice” sufficiently motivates individuals to take on those behaviors or diets.
Further, even if it is an “academic question,” these studies have yet to address what you want them to address. These studies mostly try to answer the first “academic” question by looking at the second question (which is precisely why they are flimsy and bad). So these studies actually are not testing “motivation” techniques, which makes the conclusion “the answer so far seems to be no,” misplaced.
Perhaps it’s “unclear,” but piecing together the literature allows reasonable inferences that it will.
Guilt is a strong prosocial motivator. http://www.dartmouth.edu/~thlab/pubs/97_Estrada_etal_Guilt.pdf
Shame a more powerful motivator than pride in mobilizing voters. http://link.springer.com/article/10.1007%2Fs11109-010-9114-0
Endogenous shame (shame that is directly applicable to the current decision) motivates pro-social behavior http://www.econ.upf.edu/docs/seminars/zeelenberg.pdf
Negative, “culturally-influenced” body image influences “disordered eating.” http://psy.haifa.ac.il/~ep/Students_Post/Projects/Project_1/2010-11/nollfredrickson1998.pdf
Moreover, the one study I could find that supposedly indicated that “fat shaming” was ineffective, was itself, unsurprisingly, poor.
Now, “guilt” and “shame” are technically different. Shame results from a feeling that the self is fundamentally flawed. Guilt results from the feeling that, while one could do otherwise, one fails to do so. Shaming that implants the belief that weight-control is within an individual’s control, could also contribute to individuals responding based on “guilt” rather than shame.
@Insider:
I feel this conversation is running its course. Please think carefully before any future replies, to assure whatever concern of yours was not addressed by me previously here or elsewhere.
That said:
But those same lab interventions also show that after losing weight after monitored feeding, the sensation of significant hunger does not diminish, and the subjects eventually regain the weight. Obesity appears to be a result of a form of homeostasis, as the body tries to maintain a certain level of body weight. That level has been set, in some people, at a higher weight and body fat percentage than in the past by whatever environmental factors that drove the increase in the obesity rate.
Assuming that employing some form of shaming will reduce obesity is at best speculation, the examples you give are far from definitive. Again, it is based on the idea that excessive eating is the root problem, and not something like a bodily set point. “Laboratory” overfeeding experiments also serve to challenge the notion that simple overeating is the problem. (I will add a section on these to the page at some point).
And finally you haven’t addressed a point that no one here has managed to address adequately. Even if “shaming” would work, why should we institute it? Such a policy would incur costs. Best case scenario, we have a benefit that’s purely aesthetic. Hardly worthwhile I would say.
@JayMan
Fat shaming doesn’t work.
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0070048
Since the obesity problem is recent obviously its because behaviors changed or something about the physical or cultural environment changed. Obesity is genetic only in the sense that in environments encouraging certain behaviors some people will become obese. Obesity is not determined in the sense that given available food, some people will become obese no matter what. That much is obvious.
Since this is true, it seems clear that if we identify what it is about the post 1980s environment that encourages overeating we might be able to solve the problem.
It seems reasonable to think that if it happened (wasn’t always so), it can un-happen, at least maybe.
We know post 80s culture is in many ways radically different from earlier times (the real divide is the 60s but there is always a time lag) and the movement was towards permissiveness and dropping of standards across all fields. We know that the types of food people eat is not what has changed (wonder bread was invented in the 20s) nor is the amount of food that is available what has changed.
We further have a wealth of anecdotal data (would love to see studies of this) of French and Asian students coming to America to study for a year or more and rapidly gaining 10-20 lbs, and losing it upon returning home, and Asians who assimilate into the American mainstream and drop their traditional cultural habits or are no longer exposed to Asian peer pressure tend to be fatter than Asians who remain unassimilated.
All this adds up to a picture that while obviously obesity is genetic, only in the trivial sense that I am genetically predisposed to lose my head if someone chops it with a sword – can you say I lost my head because of genetics or because someone swung a sword at it?
@Rob:
Well, that depends on what you mean by “available” food. Clearly the food availability today (and perhaps other unknown forces in today’s environment) inevitably causes some people to become obese.
It seems clear. Good luck doing that, though.
Possibly. Though keep in mind undoable in theory doesn’t mean undoable in practice (e.g., birth control).
Indeed. In what ways, we don’t know.
I’d like to see studies too. I have looked at long-generation Asian Americans and found that they are quite thinner than American Whites. American “environment” only goes so far.
Well, the environment, with regards to obesity today is essentially a constant. So it doesn’t matter that the absolute level of obesity can be modulated by environmental changes. For all intents and purposes those predisposed to obesity should regard it as a sealed fate, for the most part.
Commenters: (don’t worry, the intended people know who they are) if you’re going to preach the gospel, despite facts to the contrary, do it somewhere else.
Jayman. This is excellent work. One thing I’m curious about is the work on *intense* exercise. Such studies must exist in e.g. prisons, and in the army. Selection bias no doubt exists, but is it possible that the reason exercise is ineffective is that our standards of what constitutes exercise are just too low? No doubt the propensity to do exercise in our society is also very heritable, but it would raise the possibility that by altering the environment to encourage regular, intense exercise, we could change obesity levels.
Dermot,
Jayman has stated before the truth that exercise does NOT cause weight loss. The idea that exercise causes weight loss is a myth promoted by the exercise industry for profit, people who love going to to the gym and wish to congratulate themselves for being thin (which is more biological than the result of anything they have done), and fat shamers because they desperately want something to work to magically turn naturally fat people thin.
How is it that the body retains fat when a person enters ketosis (as in a ketogenic diet) and their body begins to rely solely on fat stored in adipose tissue?
@Antony:
Because, apparently, it’s not quite so simple.
We don’t know as much about how the body works as we think we do.
Well, I read Dr Atkins when I was 19 (1969) and he made sense to me. Said the heart attack epidemic and the growing diabetes and obesity figures were due to eating processed sugar and flour.
I went Atkins @85< carbs/day(I was lucky my metabolism could stand alot of carbos); dramatically increasing my calories but kept my weight even, cheating only once a week with sweets.. Then family and career came and I let myself go from 6'4'', 231 to 312.
April, 2000 I remembered the good Dr. and lost 81 lbs in 4 months eating more calories than during my obese days. Still today at 6'4'' 231. Just eat a little less with age as my food desire is less.
I didn’t see anything in the study about the initial weight and body composition’s correlation with the final result.
Individuals with lower body fat have substantially higher RMR’s than those with higher body fat. So we’d expect them to gain less weight anyway.
Do these diets fail because people cheat/misreport/lie? The few studies I’ve seen seem to suggest this.
Is there any evidence that people who eat fewer calories than they burn every day will not lose weight?
If so, then we’re not dealing with an “obesity” problem, we’re dealing with a population of people who lie, cheat, or have no self-control.
@Robert,
The effect is the same, is it not?
Yes, the effect is the same, but a dose of reality may help the Fat. There are some dangerous movements afoot, like “Health at Any Size.” And many Fats believe things that are physically impossible, like dieting makes you gain weight because of “starvation mode” or other crackpot nutritional theories.
Fat people may be more successful dealing with, or at least accepting, that 1) they’re not healthy and 2) their problem is self-control or cheating and not metabolic.
@Robert:
Like the other silly commenters before you, you don’t get that the issue then is equally unchangeable. Willpower doesn’t grow on trees. And even beyond that, once again, losing weight doesn’t make you any healthier.
See:
This is getting dumb, so please think carefully before commenting again.
Restricting calories along with increasing energy expenditure will lead to a decrease in weight, period. The human body stores energy as muscle and fat, so taking in less energy and using up more energy will cause the body to store less, because there is less of a surplus. So it seems like the dispute is over whether people can be motivated to lose weight.
Even assuming “willpower” is unchangeable, taxing certain ingredients or foods could shift dietary patterns. In turn, there could be government entitlements given to individuals who exercise a certain amount everyday, funded by the tax revenue. Are there any studies you have on willpower that show it has a high h^2 and is relatively immalleable?
The studies you rely on to support your claim that obesity has no impact on health seem like t ypical self-report studies and aren’t worth much, if anything. Here’s a review that states that, metabolically normal obese individuals are still less healthy than metabolically normal thin individuals. It has a few flaws, though.
http://annals.org/article.aspx?articleid=1784291
@Swank:
You are one comment away from being banned. Think very carefully about your next reply.
That’s technically true but not really meaningful. How do you control energy expenditure, for example? It’s hardly as simple as it sounds.
See:
Fat Head » Toilet Humor And The HOW vs. WHY Of Getting Fat
The Physics Diet? | Slate Star Codex
There’s one referenced on the page.
No, that’s not what I rely on. I rely on the correlation between IQ and health/lifespan, as well as the (inverse) correlation between IQ and BMI. This, and the problems with the crap study you cited, were explained on the page.
Like I said, you’re one comment away from being banned. I have zero time for people who can’t even read the thing they’re critiquing.
Ok, assuming the study implies immalleability, people can still make their low self-control work to their advantage: set up automatic billing for delivered foodstuff and get rid of all food in the residence (or pay someone to do this). And government taxation could work. You say “assuming behavior is the problem.” People eat more now than they did 60 years ago, they weigh more than they did 60 years ago, and eating more food has a clear link to weight gain. So the behavior of eating more seems to be a plausible candidate for the problem, or a significant part of the problem.
The general fitness factor/g/cognitive epidemiology stuff is interesting. But IQ is correlated with myopia and BPD, as well. Is that explained anywhere?
@Swank:
We still have a key problem: we don’t know the root cause of why people have gained weight. This is true even if people are eating more these days, because the question then becomes why? Without knowing the root cause, we can’t reliably come up with a solution.
There has been a documented increase in the proportion of omega-6 polyfats versus omega-3 polyfats in our diets as a result of processed food. Europe does not have this same imbalance, and Europeans weigh less. Omega-6 has been linked to hypothalamus appetite control.
So, we know that processing methods are linked to our appetites. We know that we eat more. And we also know that we are less active.
So, 1) eating less should help, 2) avoiding processed foods should help, and 3) exercising should help (people are less active now than they were then).
@Swank:
We can produce a million correlations. They don’t necessarily tell us about the cause.
As for the rest, it’s been addressed a million times before on this very page. I’m done with it. No further comments (from anyone) that are egregiously stupid will be approved here.
There are many studies about conditions that have comorbidity with Obesity:
http://www.wvdhhr.org/bph/oehp/obesity/commor.htm
It’s hard to believe your statements saying that the Fat are no less healthy than the Normal-Sized.
@Robert:
Oh for fuck’s sake Robert, reread the goddamned page.
One more stupid comment and you’re banned.
It could be a combination of genetics and diet if particular populations *process* particular foods differently and the proportion of those particular foods has increased in the diet of the populations not adapted for them.
The obvious candidate here is sugar.
Populations with the longest history of grains as the staple in their diet (i.e. populations from the earliest farming regions) may be more adapted to the sugar in grains and so less effected by the sugar added to processed foods.
Populations with the shortest history of grains as the staple in their diet would be most effected e.g. North Europeans, Africans, Native Americans etc.
The same effect – if it exists – might have some connection to alcoholism.
One possible mechanism for how different populations might process different food types differently is if some populations fully register their sugar intake as food and some don’t.
e.g. a pie 1/3 meat, 1/3 fat and 1/3 sugar
Someone fully adapted to sugar might register all three and feel full sooner.
Someone not adapted to sugar might not register the sugar part and so only feels full when they have eaten enough of the meat and fat so they eat 50% more calories than they need.
(Obviously very simplified example.)
Any thoughts on what the Nutrition Science Institute (NuSI) is doing? ISTM that they have their collective head screwed on mostly straight (Taubes practicing what he has been preaching) but I don’t see it mentioned here. I personally find Taubes’ hypothesis in “Good Calories, Bad Calories” compelling but am hoping that NuSI will succeed in getting actual reliable data in the not-too-distant future.
Most of the rise in obesity we’ve seen has been over a period of 40-50 years.
How did the genetics of body weight change that quickly?
@Anonymous:
They didn’t.
So by what process do the same genes produce reasonably fit people 50 years ago and obese people today?
@Anonymous:
Figure that out and you might just be able to claim a Nobel.
Our diets have changed over 40 years if you don’t understand how that affects a population of animals you don’t understand ecology
I’m not sure anyone really does.
Interesting article at Slate on obesity and the failure of diet and exercise from March 2015:
http://www.slate.com/articles/health_and_science/medical_examiner/2015/03/diets_do_not_work_the_thin_evidence_that_losing_weight_makes_you_healthier.single.html
Here is another recent piece. This one is from the Washington Post and is an interview with a scientist who studies weight and obesity. Her conclusion is that diet doesn’t work at all and is even counterproductive: http://www.washingtonpost.com/news/wonkblog/wp/2015/05/04/why-diets-dont-actually-work-according-to-a-researcher-who-has-studied-them-for-decades/
Amazing! I first got a lot of this information (without references) from http://www.thefreelibrary.com/All+this+yammering+about+obesity+a+big,+fat+lie.-a0117213868
Has anyone tried to estimate the BMI of prehistoric hunter-gatherer people? In many modern HG societies the adult BMI is only about 20 but these people may not make the best models for prehistoric people since they live in marginal habitats like semi deserts or poor woodland and have quite poor diets. Has anyone tried to estimate BMI from bones or something? Thanks.
Alright, so what do you make of this? Title: ‘Leisure-time physical activity and intra-abdominal fat in young adulthood: A monozygotic co-twin control study’. Results: ‘Inactive twins had 31% more intra-abdominal fat than their active co-twins (mean difference 0.52 kg, 95% CI 0.12 to 0.91, P = 0.016)…’ Conclusion: ‘A lower level of physical activity is related to greater accumulation of intra-abdominal fat among healthy adult males in their mid-30s. The findings highlight the importance of leisure-time physical activity independent of genes and diet in the prevention of intra-abdominal fat accumulation from early adulthood onward.’
p.s. – you list Inductivist in your “defunct blogs” section, but as of Jan. 3rd ‘16, it looks like he’s begun posting again.
N = 10 pairs. ‘Nuff said, though there are numerous other problems here.
Jay do u know who controls the biggest experiments? Its the people wiping the butts of the corn industry/politicians. We live in a bought for, rigged scientific arena thanks to our politics today. This is all research akin to big tobacco declaring cigarettes did no harm. They had studies to prove them. You confuse studies with evidence. Why can’t aedon find a study that duplicates that experiment? Its because they don’t fund it. Those studies that people like us want funded show that were poisoning ourselves and its BC that’s what the corporations are selling us. We must fight for real quality meats and fish, not to mention clean water, do u know how many ppl in the us don’t have clean water?
Actually:
http://www.overcomingbias.com/?s=smoking+trials
As someone who was fat their whole life but was very athletic at the same time, when i changed my nutrition to a high fat high protein diet my body type shifted dramatically. I think nutrition has been backasswards for centuries now. Metabolically speaking we need to train our bodies to produce and burn ketones for energy rather than sugar for energy. Sugar is meant to be fat, anyone who knows insulin pathways agrees with this. protein is meant for muscle . Fat is meant for energy to be produced in the form of keytones, but it is also essential for numerous other essential metabolic activity (hormones, tissue structure, etc) we have little to no real understanding of the role o macromolecules after they are ingested in animals.
I think you could have just posted that, and eschewed the rest.
Hey JayMan. A few things I’ve come across you will find interesting if you haven’t seen it before.
Blüher (2012) reviewed the data on obese patients and found that 30 percent of them were metabolically healthy with the obese patients having similar levels of insulin sensitivity similar to lean individuals.
http://www.ncbi.nlm.nih.gov/pubmed/22895358
This one should chang what we think about BMI:
In a huge study of over 120,000 people, the researchers gathered people from Copenhagen, Denmark, recruiting people from 1976 to 2013. They were then separately compared to those who were recruited in the 70s, 90s, and 00s. Surprisingly, the BMI linked with the lowest risk of having died from any cause was 23.7 in the 70s, 24.6 in the 90s, and 27 from 2003-2013. Due to the results of this study, the researchers are arguing that BMI categories may need adjusting.
http://www.ncbi.nlm.nih.gov/pubmedhealth/behindtheheadlines/news/2016-05-11-bmi-categories-may-need-adjusting-argue-researchers-/
Great research.
JayMan,
I started reading Good Calories, Bad Calories by Taubes. I read Rethinking Thin by Kolata, Why Diets make Us Fat by Sandra Aamodt And The Obesity Code by Jason Fung. I have Why We Get Fat and What to Do About It by Taubes to finish after GCBC. Secrets of the Eating Lab by Mann just got to my house today (the author of the study you cite with Mann and Tomiyama.
My mind is forever changed on dieting. I also get what you said to me about a decrease in expenditure when dieting a few months ago.
Solid posts man.
Also, about metabolism. Have you seen the Vermont Prison Study?
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC292021/pdf/jcinvest00194-0053.pdf
They were fed up to 10k kcal a day, and their metabolism increased by 50 percent in an attempt to burn off the excess kcal.
Also what are your thoughts on the First Law of Thermodynamics in regards to human physiology? And what are your thoughts on the NuSI study funded by Taubes, with Kevin Hall spinning the data?
https://www.dietdoctor.com/how-kevin-hall-tried-to-kill-insulin-hypothesis-pure-spin
https://proteinpower.com/drmike/2016/05/06/contradictions-and-cognitive-dissonance-the-kevin-hall-effect/
Great summary of the literature looking at the high level non-impact of the diet and exercise conundrums. A couple of things you may want to consider. As a doc I can say more of us have changed our minds in the past decade than you think.
Perhaps the most important paper in the past decade is here
Persistent metabolic adaptation 6 years after “The Biggest Loser” competition
http://onlinelibrary.wiley.com/doi/10.1002/oby.21538/abstract
This has placed the dagger in the dieting myth on multiple levels.
At a very basic level weight gain is the difference between calories in and calories out. As you are aware the standard advice is calories in are limited by portion control. Calories out is increased by exercise.
You have the data to show why this is not true in general. The fact is 30 min of cardio burns 200 calories (approx) to get 1 lb a week off somebody is a close to 800 calories per day. Your choices are 2 hrs of cardio a day vs reducing calorie intake. As I say to my patients weight loss is ALL DIET and marginal exercise.
Ok. So your data says that doesn’t work well in a global sense. So the next question is the interplay of metabolism and calories.
There is subtlety buried in the weight gain = calories in – calories out
First, I need to bust a couple of myths.
1) all calories are NOT created equal
2) basal metabolic differences DO exist, and change over time
Calories are not equal. They are in a calorimeter but not in your body. Unfortunately the assumption that calories are equal drove nutrition science for most of the past 70 years.
Overall calories in is determined by the food density impact on your satiety. What this means is that you need to eat foods that make you feel full. Sounds simple but this is the crux of the matter. You have to eat a calorie restricted diet that fools your body into thinking it had a more filling meal vs other calorie sources.
This was figured out in the early 1980’s through 1990’s.
The first challenge to not all calories are equal was the glycemic index develop in the early 1980’s in Toronto and Sydney. There are some issues with the measurements but in showed how an individuals body responded to different food loads. The trouble was it varies between people and did not help answer the question how you felt. It did show rice cakes/soda are a terrible choice since you feel increased hunger after consumption due to the sugar crash.
The next part is the Satiety Index developed in 1995 in Sydney ( I got to sit through her lectures right after it was published).
At this point in time cutting edge diet work puts these concepts together to look at the impact of the macromolecule mix. The basic upshot is – oatmeal is almost the best breakfast food ever, the French sequence of salad, followed by soup, then a small protein load and cheese eaten over 60 min is probably genius.
The other side of the equation is a basal metabolic set point. Of course it varies as you age (you slow down), to such a degree you won’t find a 90 yr old with a BMI over 25 (they all die). It also is environmentally impacted. The biggest loser data shows that after a major metabolic reset – your body will NEVER RECOVER. The lower metabolism set point leads to continuous weight gain at a LOWER overall calorific intake. That is problematic for a yo-yo dieter.
Sugar, carbs and fat are not evil. From a nutrition perspective evil is anything that has high energy density with sharp blood sugar spikes and is non-satiating.
No idea how you change this on a population basis
I’m old. We didn’t have that many really fat people in the olden days. Even the poor, in the days of The Grapes of Wrath, were gaunt and thin. Now the poor are generally bulbous and pear shaped. The genetics can’t have changed that much in two generations.
No one said they did.